
Prevention and Management of Malaria in Children using a School-Based Program Model
Malaria continues to be a major cause of mortality and long-term neurologic handicap globally; the burden of disease is particularly high among children. Those living in rural and poorly resourced areas of the world are the most severely affected, in large part because of inequities in health care for malaria that impact children. School-aged children are a subset of the at risk population who are particularly vulnerable to the adverse consequences of delayed diagnosis, sub-optimal care and repeated infection; both the short and long-term neurologic effects that can result are recognized to compromise the learning ability of affected children. Because of this, schools are a logical and appropriate venue for focusing the fight against malaria. This photo essay illustrates how an effective intervention in rural African schools combines the parallel implementation of a prevention strategy based on the promotion of bed net use by pupils, with a teacher-driven strategy to diagnose and treat malaria through the use of rapid diagnostic testing and artemisinin combination therapy. Strategies such as this reduce inequities in care and offer a way to reduce morbidity from malaria; this in turn gives school children a greater chance of achieving their academic potential by avoiding both absence from school and the long term effects that malaria can have on their ability to learn.
1. Introduction
Malaria is an example of an infectious disease that is preventable but can devastate the life of a child when infection occurs if the disease is not diagnosed appropriately and treated without delay; adverse effects occur in three interconnected ways, by harming their health, disrupting their education and limiting their long-term potential. (Cohee et al, 2021) Malaria disproportionately affects those living in remote or resource-poor rural communities (Barat et al, 2004), and consequently malaria is a significant problem in rural schools in Africa. The rates of infection among pupils are high, in large part because many parents in these communities do not understand that mosquitoes cause malaria, that infection can be prevented, and that diagnosis and treatment are needed promptly. Additionally, clinics in rural areas are limited in number, so the distance to reach them plus the cost of treatment can mean that even parents who do understand that their children need medical care, may still not be able to get the management recommended by the World Health Organization (WHO), which is accurate diagnosis and effective treatment within 24 hours of illness onset (WHO, 2022).

Pupils arriving at a rural primary school in Uganda. The principal reason why a child will be absent from school in Africa is infection with malaria; without prompt treatment most are absent for many days, and often for a week or more.

A child with symptoms of malaria. Children found to be sick at school are traditionally sent home to be cared for by their parents. Delayed or inappropriate treatment results in prolonged symptoms; such children often struggle to pay attention and learn when they return to class.
2. The impact of malaria on child health and educational potential
Repeated episodes of infection are common and recurring periods of absence mean that affected pupils quickly fall behind in their studies. Children who are not treated according to WHO guidelines also often continue to have symptoms that prevent them from participating fully even when they feel well enough to return to school (Nakitende et al, 2023).
Children risk failing to succeed academically when they have repeated episodes of infection, and malaria is a major cause of children dropping out of school. The long term consequences of infection can be serious; adverse effects on the brain can reduce a child’s ability to concentrate which cause difficulty with learning and retaining knowledge, and children can also be left with serious long term neurologic handicaps. Malaria is also the principal cause of death in school-aged children in Africa as those who become infected can deteriorate and become dangerously ill in a matter of hours.
3. Schools as focus for innovative intervention and essential education
If malaria control interventions are to achieve their desired impact, they must reach the least well served segments of the population. Programs designed to provide prompt diagnosis and treatment of children in rural schools are an important way to remedy the inequities in access to care known to occur in sub-Saharan Africa and other areas of the world where malaria is endemic (Macnab, 2026).
Schools are an obvious location for interventions to improve malaria care for children (Temperley et al, 2008), however, programs that focus on the needs of children in this regard are limited, in spite of there being many examples of other school-based health initiatives that can be delivered in a successful and cost efficient manner (Macnab, 2026).
Including education about malaria in the school curriculum is necessary as many school children lack the knowledge required to reduce their risk of infection and manage symptoms of possible disease. Forming malaria clubs in schools is another constructive strategy. Membership in these clubs should recognize and acknowledge all the pupils who learn what causes malaria, that it can be prevented and the importance of early diagnosis and treatment. Club activities can also be used to sustain active participation in school-based programs and encourage the active engagement of pupils in the promotion of malaria awareness and outreach into their community.

Members of the school malaria club wear a T shirt designed to recognize their commitment, encourage other pupils within the school and promote the program during activities with other schools and in their community
4. The importance of prevention
In addition to in class education explaining the purpose and importance of measures that help prevent malarial infection, our program particularly stresses the importance of bed net use by participating pupils. This follows evidence that rates of ownership and use of insecticide treated bed nets is low in rural Uganda.

Strategies to improve prevention should include awareness of how important it is to sleep under a protective bed net. Hence, when starting a school-based malaria program a necessary component is to explore the logistics of how best to provide treated bed nets and promote their consistent use.

In our program a team from the Department of Family Practice at Makerere University works with teachers to make them aware of the problems associated with malaria and how to prevent, diagnose and treat infection. Teachers welcome this as a way to improve the health and academic potential of their pupils.
In our experience, an important and constructive adjunct to school-based malaria education and care isthe addition of strategies that provide bed nets in parallel with other interventions; this is particularly importantin programs involving boarding schools. Such initiatives should provide a way for schools to help parents to buy nets, perhaps through a subsidy; this is because net purchase, even for a minimal fee, generally leads to moreconscientious use than where nets are just handed out for free.

School-based programs are important as the WHO has emphasized that the recent advances that have made malaria vaccines available are a reason to reinvigorate efforts to reduce the burden of the disease among children, and not a substitute for such interventions.
5. The World Health Organization calls for improved diagnosis and care
The WHO continues to call for multi-faceted programs able to complement the current efforts to begin vaccination in pre-school age children (Macnab, 2021). For this reason we suggest school-based programs should be scaled up to engage with pupils to educate them about malaria, increase their awareness about how it is caused and emphasize the importance of prevention, as well as providing teacher-driven testing for all children found to be sick at school. In this way treatment can be provided without delay for all those testing positive for malaria, and with increased awareness about the disease and its consequences, the burden of disease on children can be progressively reduced.
Providing an intervention for malaria that is based in a school and empowers teachers to ‘test and treat’ means that treatment can be provided without delay for all those children who are found to be ill at school and who test positive for malaria. Importantly this provides care that meets the WHO’s mandate for appropriate management of malaria; namely, accurate diagnosis and effective treatment within 24 hours of the onset of illness. (WHO, 2022) In addition, as well as improving the care of individual children at the school, programs like this offer a way to progressively decrease the burden of disease in the broader community, because the overall number of individuals infected with malaria parasites is reduced, and the educational components delivered in parallel to acute disease management increase awareness about the disease and its consequences.

School-based programs should be structured to engage pupils so as to educate them about malaria,increase their awareness about how it is caused, and emphasize the importance of prevention. In addition, wesuggest they should provide teacher-driven testing for all children found to be sick at school.
6. Insecticide treated bed nets
The prevention provided by treated bed nets against being bitten by mosquitoes that carry malaria is now well understood in the schools where we have programs in place, and as a result most children now sleep under a bed net. In areas with stable malaria due to Plasmodium falciparum, ITNs reduced the incidence of uncomplicated malarial episodes by 50% compared to no nets, and in areas of unstable malaria by 62%; for Plasmodium vivax episodes, ITNs reduce the incidence by 52% (Lengeler, 2004). Importantly, it has been shown that regular and correct bed net use is more likely when an education program about how malaria is spread and why ITN’s provide benefit accompanies campaigns that provide bed nets (Polec et al, 2015).
7. Rapid diagnostic tests (RDT) and Artemisinin combination therapy (ACT)
The rapid diagnostic test kits (RDTs) and treatment with artemisinin combination therapy (ACT) that we teach the teachers to use are WHO-approved. Both have been extensively validated (Steketee et al, 2017), and consequently their use in combination for accurate diagnosis and prompt treatment is central to most national malaria management strategies. But despite this, the burden of disease remains unacceptably high in rural areas and other low-resource settings where access to these interventions is limited (Macnab, 2026). However, programs like the one we describe are an example of school-based health promotion initiatives that can benefit children and reduce the burden of malaria significantly (Macnab, 2026).

In the boarding schools in our program, the dormitories now have insect treated bed nets (ITNs) able to protect children sleeping in bunk beds in addition to those suitable for use over individual beds. This practical step improves the level of protection available.

The preventive element that bed nets provide now complements the role teachers have as care providers in our programs. Teachers are trained how to do a rapid diagnostic test for malaria on any child who becomes sick; this simple test involves taking a finger prick blood sample; teachers then administer treatment without delay to those testing positive.
8. Interdisciplinary collaboration
Collaborative school-based programs bring together the experience and commitment of teachers and the knowledge and skills of health care providers. This collaboration is a logical, straightforward and inexpensive way to respond to the consistent and continued calls to improve malaria care for school-children (Nankabirwa et al, 2014): WHO, 2022; Macnab, 2026). Innovative practical approaches like this are particularly needed to improve the unacceptably high rates of mortality and morbidity from malaria among children living in rural communities where the burden of disease is known to be greater than for those in urban areas (Duodu et al, 2022). Schools are an obvious location to focus care for children at risk. Our observation of how willingly and effectively teachers can be engaged and trained as front line providers of essential elements of health care corresponds with prior literature reporting the effectiveness of school staff in other health delivery roles (Macnab, 2026). Our confirmation that teachers can be trained to recognize and respond appropriately to the emergent needs of children with signs of severe illness is further strong evidence of their place in future efforts to improve malaria care for children. Finally, we suggest that the program model we describe is also an example of a practical pathway that family practitioners can use to introduce and promote improvements in care as part of their role as health care providers in the community.
In addition to being a logical way of scaling up access by children to nationally advocated malaria management using RDT and ACT, this school-based intervention gives school-aged children the best possible chance to benefit fully from their education and achieve their academic potential.
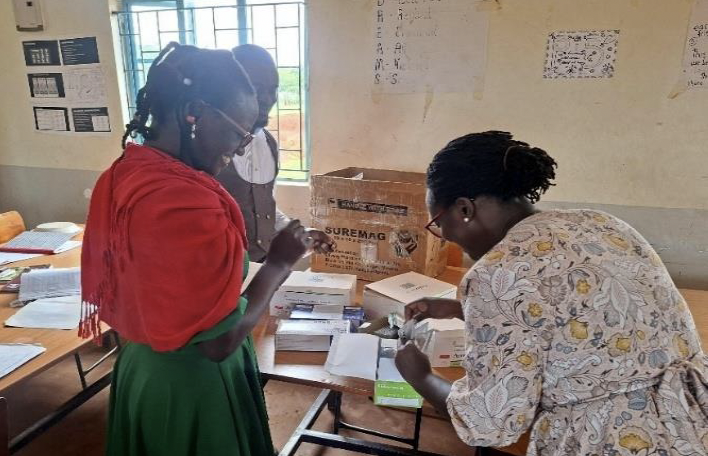
Teachers and members of the Family Practice team learn from each another. One important skill the teachers have learned is to how to recognize when a child’s symptoms indicate that she/he is developing a severe form of malaria. This enables such children to be hospitalized without delay for intravenous fluids and medication; such recognition and prompt action can be lifesaving.

Preventive strategies involving bed net use combined with teacher-driven diagnosis and care offer a proven way to reduce morbidity from malaria.
9. Conclusion
If malaria control interventions are to achieve their desired impact, they must take into account how social determinants of health negatively impact the care of school-aged children and provide services that reach the least well served segments of the populations (Barat et al, 2004). In this context, school-aged children have long been recognized to be underserved (Nankabirwa et al 2014; Cohee et al , 2021), and consequently suffer a disproportionately high health burden from the disease. Importantly programs like ours are likely to have broad benefit; school-based health promotion has been shown to contribute towards achieving elements of the UN sustainable development goals (Macnab and Mukisa, 2017), and a recent metanalysis identified that school-based malaria prevention can improve cognitive and educational outcomes at low cost. (Angrist et al, 2023). Consequently, in addition to improving children’s health, school-based teacher-driven malaria intervention offers important social benefits, can be cost-effective, and through the educational benefits achieved, offers children a greater chance to achieve their full potential.
“Globally, a moral imperative exists to ensure that all children and adolescents are provided with the resources
and environment necessary to enable them to reach their individual potential”
Acknowledgment
We acknowledge the collaboration and many contributions of the teachers and pupils at the schools where we work. Also, the funding provided for this project by Rose Charities Canada and the Hillman Medical Education Fund.